

This guide to auscultating lung sounds will cover everything emergency medical technicians (EMT) need to know about assessing a patient’s breath sounds. Lung auscultation is an important medical skill that EMTs and paramedics should be familiar with. You will learn about the anatomy of the lung along with landmarks for lung auscultation. This article will also cover the different types of breath sounds and provide sample audio clips of adventitious lung sounds. Lastly, you can find tips first responders can use to become better at auscultation in the field.
EMTs and paramedics in the field may find it especially difficult to assess a patient’s breath sounds because of the noisy environment and constant movement. There are steps you can take to make sure you get the best reading every time you place your stethoscope and listen to a patient’s lung field.
An important step is to place your stethoscope’s diaphragm on the correct areas of your patient’s chest and back, so you can clearly hear air moving through the passageways.
Types of Lung Sounds
Breath sounds can be categorized as normal and abnormal. Abnormal lung sounds that have additional noise when listening are called adventitious lung sounds.
Abnormal lung sounds include:
→ Wheezing Lung Sounds
→ Rhonchi Breath Sounds
→ Stridor Lung Sounds
→ Crackles Lung Sounds (Rales)
→ Pleural Friction Rub
→ Diminished Breath Sounds
→ Absent Breath Sounds
Wheezing, rhonchi, stridor, crackles and pleural friction rub are all adventitious lung sounds because you will hear extra noises in the airways during the assessment. Absent and diminished breath sounds are also abnormal, but they are not considered to be adventitious lung sounds.
Normal lung sounds include:
→ Vesicular Breath Sounds
→ Bronchial Breath Sounds
→ Bronchovesicular Breath Sounds
Most of the breath sounds videos in this article are meant to be listened to with headphones. They were taken using the Thinklabs Digital Stethoscope. You can check out the website and hear more breath sounds and heart sounds at https://www.thinklabs.com/lung-sounds.
Wheezing Lung Sounds
(This is a 7 month-old patient with bronchiolitis. The soft mid-inspiratory and mid-expiratory wheezes heard in the video suggest a bronchiolar disease.)
Wheezing lung sounds are one of the easier to identify breath sounds for EMTs and paramedics. The wheezing sound can be heard during inhalation or exhalation and it’s caused by a narrowing of the airways.
Wheezing lung sounds are continuous and can be heard throughout the lungs. They have a musical quality and are often caused by bronchospasm. The term “classic wheeze” refers to a high pitched whistle during expiration.
Conditions likely to produce a wheezing sound.
• Asthma
• Bronchitis
• Allergic reaction
• Inhaling a foreign object into the lungs
• COPD
• Pneumonia
• Smoking
• Heart failure
Rhonchi Lung Sounds
(This patient is intubated with atonal, low-pitched rhonchi.)
Rhonchi breath sounds are a lower pitched wheezing sound. Rhonchi sounds are continuous and can sound like snoring or even have a moaning quality. They are caused by air passing through airways that are narrowed due to secretions or mucous.
Rhonchi sounds may be describes as sonorous wheezes heard in the smaller airways. An important feature of rhonchi breath sounds is that they will often clear up after the patient coughs or is suctioned. They can be heard during inspiration and expiration.
Conditions likely to produce rhonchi sounds.
• Chronic bronchitis
• Pneumonia
• Cystic fibrosis
Stridor Lung Sounds
(Stridor in an infant.)
Stridor lung sounds are frequently heard in children and are caused by something blocking the larynx. Stridor breathing is continuous and tends to be one of the easier adventitious lung sounds for EMTs to recognize.
It is a high pitched musical sound heard on inspiration that’s caused by air moving through a partially obstructed airway. Often it will be possible for first responders to hear stridor breathing without a stethoscope.
The stridor sound can be mistaken for wheezing, but there is a simple way to check whether the patient is experiencing an inspiratory wheeze or stridor. EMTs can use their stethoscope and gently listen over the patient’s throat (trachea) for the stridor sound to get louder. If the breath sound increases at the throat, the patient has stridor breathing and not an inspiratory wheeze.
Stridor breathing may indicate a medical emergency in patients who are not getting enough oxygen.
Conditions likely to produce stridor breathing.
• Croup (laryngotracheobronchitis)
• Foreign body airway obstruction
• Laryngospasm
• Swelling in throat
• Epiglottitis
Crackles Lung Sounds
Crackles lung sounds can be trickier for EMTs and paramedics than other adventitious lung sounds for a variety of reasons. Crackles lung sounds can be categorized both by the sound quality and when they are heard in the respiratory cycle. Crackles can occur on inspiration or expiration and each type can indicate a different disease process.
Other reasons that crackles breath sounds can trip up first responders are: they can sound similar to rhonchi, they were previously called rales breath sounds, and people often describe crackles using terms like dry, moist and wet.
Coarse Crackles
Coarse crackles are a crackling sound when breathing that is usually caused by mucous in the airways. Course crackle lung sounds tend to be a loud, low pitched bubbling sound.
They can be heard anywhere in the anterior or posterior lung fields and it’s also possible for coarse crackles to be heard on one side of the chest, in both lungs, or in different spots throughout the lungs. Course crackles in the lungs can also be described as rattling, gurgling or cracking sounds heard with breathing.
(This is a 47 year-old male patient with course crackles from bronchiectasis.)
Conditions likely to produce course crackles in lungs.
• COPD
• Bronchiectasis
• Lung Abscess
• TB lung cavities
• Pneumonia
Fine Crackles
Fine crackles lung sounds are discontinuous, high pitched popping sounds. As air rapidly opens the collapsed air sacs in the lungs, it can produce a popping or crackling noise. Fine crackles tend to be brief and sound like wood burning or like the crumpling of cellophane. You can also rub dry hair between your fingers and close to your ear in order to get an idea of what fine crackles sounds like.
Unlike course crackles, fine crackles will usually start at the base of the lungs where fluid congregates. As fluid fills the lungs, fine crackles lung sounds will be heard higher up in the lungs. Fine crackles in lungs won’t clear when the patient coughs.
(This is a 21 year-old adult male patient with Cystic Fibrosis. You can hear both Fine Crackles and Wheezes in this video.)
Conditions likely to produce fine crackles in lungs.
• Pulmonary edema
• Bronchiolitis
• Cystic fibrosis
• Consolidation
Pleural Friction Rub
A pleural friction rub occurs when the inflamed pleural surfaces rub against each other during respiration. EMTs and paramedics can hear the sound of a pleural friction rub both on inspiration and expiration. Often it can be heard at the end of inhalation and the beginning of exhalation.
It can be described as a low pitched creaking or grating sound in the lungs. A pleural friction rub often sounds like boots walking on fresh snow or like the sound of leather rubbing together. In the field, a pleural friction rub can sound similar to a pericardial friction rub.
An easy way to figure out the difference is by having the patient hold their breath while you listen with your stethoscope. If you can still hear the rubbing sound, than it’s the heart and not a pleural friction rub. Often the sound of pleural rubs can be localized to a specific location in the lung and chest area. Pleural friction rub sounds can be continuous or broken and will be heard every time the patient takes a breath.
(This is a predominately inspiratory low frequency sound. This pleural friction rub is an example of one that sounds similar to rubbing pieces of leather together.)
Conditions likely to cause a pleural friction rub.
• Pleurisy
• Pneumonia
• Pulmonary Embolism
Diminished Lung Sounds
Diminished lung sounds are considered abnormal, but they are not classified as adventitious lung sounds. However, both adventitious lung sounds and clear breath sounds can be diminished. This just means they are muffled or are at a lower volume than expected. The important thing is to determine why the patient has diminished lung sounds and whether the patient is in any danger. Diminished lung sounds are often caused by:
⇒ Increased chest wall thickness
⇒ Air or fluid
⇒ Over inflation
⇒ Reduced airflow
They are commonly heard in obese or extremely muscular patients because the extra tissue mass can impede sound.
Elderly patients may have a reduced airflow due to shallow breathing. For these patients you can get a better idea about what’s going on by asking them to take a deep breath through their mouth.
When assessing a patient with diminished lung sounds, EMTs and paramedics should compare each lung and the lung lobes to each other in order to get a clear picture of what’s going on. Diminished lung sounds can occur in one lung, both lungs, or even in different lung lobes.
Patients will often have diminished lung sounds in the base of the lungs from fluids or air obstruction. Asthma patients can have extremely diminished lung sounds instead of wheezes. This is serious and caused because the airways are so constricted that barely any air can move through the airways.
Patients who can’t move air equally throughout the lungs will commonly have diminished lung sounds. For this reason, it’s common for emphysema patients and even those with a barrel chest to regularly present with diminished lung sounds.
Diminished lung sounds can also indicate serious conditions like hypoventilation, pleural effusion, obstruction, or atelectasis. If you auscultate diminished lung sounds on one side of the chest it could indicate a pneumothorax, or collapsed lung which is a serious condition.
Conditions likely to cause diminished lung sounds.
• Pneumothorax
• Severe Asthma
• COPD
• Lower lobe consolidation
• Pneumonia
• Lung Cancer
• Pleural Effusion
• Obese & Muscular patients

Absent Lung Sounds
Absent lung sounds are a significant finding for first responders and should not be ignored. Absent lung sounds are exactly like you would expect, there will be no sound. There is no air movement through the airways for the stethoscope to pick up, which means no gas exchange for the patient.
In cases of absent breath sounds, it’s important for EMTs and paramedics to assess the overall condition of the patient. If all lung fields have absent lungs sounds, check your patient for signs of respiratory arrest. These patients will need immediate ventilation and possible intubation.
Patients can have absent lung sounds in portions of a lung. For example, the airway can become obstructed which will block the flow of air farther along in the airway. This can cause absent breath sounds in the lung lobes after the airway obstruction.
Conditions likely to cause absent breath sounds.
• Airway obstruction
• Respiratory arrest
• Atelectasis
• Lung collapse
Normal Breath Sounds
(This video has a sample of vesicular breath sounds, bronchial breath sounds, and bronchovesicular breath sounds.)
Vesicular Breath Sounds
These are normal breath sounds that can be heard throughout the entire peripheral lung field. Vesicular breath sounds are soft, low-pitched and will be heard anteriorly, posteriorly, and laterally. These are the most common breath sound and inspiration will be longer than expiration.
Bronchial Breath Sounds
These are normal breath sounds that are higher pitched and louder than vesicular breath sounds. Bronchial breath sounds can be described as hollow or tubular sounding and are only heard anteriorly, mainly over the tracheal area. Inspiration is slightly shorter than expiration with a distinct pause in between. The landmark for checking bronchial breath sounds is at the middle of the throat where the clavicles meet.
Bronchovesicular Breath Sounds
These are normal breath sounds with a low to medium pitch which usually have a soft intensity level. With bronchovesicular breath sounds inspiration and expiration time periods will be equal. These breath sounds can be heard both anteriorly and posteriorly. The anterior landmarks for bronchovesicular breath sounds are the midclavicular lines at the first and second intercostal space, on both the right and left sides. Posteriorly, you can hear bronchovesicular breath sounds between the scapula, at the T3 and T4 areas.
Lung Anatomy and Auscultation Sites
The goal of lung auscultation is to detect any missing or abnormal breath sounds. To accomplish this you need to know basic lung anatomy and the landmarks for stethoscope placement.
EMTs and paramedics should be familiar with the basic lung anatomy of both the right and left lungs. The right lung anatomy is made up of three lobes separated by the horizontal fissure and the oblique fissure. They are labeled the right upper lobe, the right middle lobe, and the right lower lobe.
Left lung anatomy is made up of two lobes separated by the oblique fissure. They are labeled the left upper lobe and left lower lobe.
Learning the location of the lungs in relation to the clavicles and being familiar with intercostal spacing will make you more proficient at patient assessment. A good way to learn this is by visualizing and listening to auscultation site landmarks on yourself, a partner or a friend.
Auscultation sites may vary depending on your training, but here are common stethoscope placement spots. I will go over eight common places to listen for breath sounds on both the front and back of patients. However, it’s common for EMTs to use six sites instead of eight. The important thing is that you listen to each lobe of each lung. EMTs should start at the apex of the lungs and make sure to listen to the base of each lung.
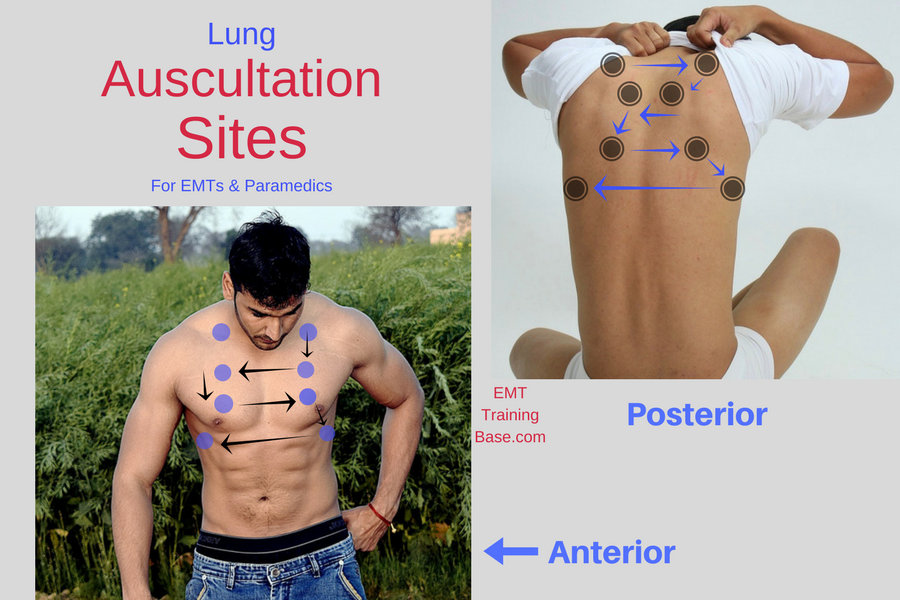
Anterior Lung Auscultation
All these lung auscultation sites can be found on the Lung Auscultation Sites diagram.
EMTs performing an anterior lung auscultation will mostly be listening to the upper lung lobes. The first responder will go to the apex of the lungs for the first two auscultation sites. First, find the patient’s clavicle and go to the midclavicular line on both the right and left side. Then go slightly above these spots and listen.
Next move down to the second intercostal space and listen to each lung at the midclavicular line. You are still listening to the upper lung lobes at these two sites.
First responders can then listen to the right middle lobe and left upper lobe at the fifth and sixth lung auscultation sites. Move down to the fourth intercostal space and listen to each lung at the midclavicular line.
The last anterior lung auscultation sites will finally assess the lower lung lobes on both the right and left sides. EMTs should move down to the sixth intercostal space and move laterally to the midaxillary line for stethoscope placement. Listen to the base of the lungs here.
Posterior Lung Auscultation
All these sites can be found on the Lung Auscultation Sites diagram.
EMTs performing a posterior lung auscultation will need to work around the patient’s shoulder blades. However, listening to breath sounds posteriorly is recommended because there are fewer bones, muscles, and organs to disrupt the lung sounds.
EMTs will start at the apex of the lungs by going slightly above the patient’s scapula around the midclavicular line. It’s best to have the patient pull their arms forward and in their lap whenever possible. This pulls the shoulder blades out of the way and gives you more room to listen to breath sounds.
Next go to T3 and listen in the space between the spine and the scapula on both the right and left side. This will assess the breath sounds in the right and left upper lungs. An easy way to get to T3 is by locating the vertebral prominens at C7 and counting from there. (See image below)

The fifth and sixth posterior lung auscultation sites can be found on the right and left sides between T3 and T10. You can listen in the space between the shoulder blades and spine to hear the lower lung lobes.
EMTs can move down and towards the midaxillary line on both the right and left sides for the last two lung auscultation sites.
How to Auscultate Lung Sounds

• Start at the top and finish at the base of the lungs while comparing the right and left sides. (See arrows on Lung Auscultation Diagram.)
• Listen to breath sounds on both the front and back of patient.
• Have the patient sitting up with arms resting in lap if possible.
• Listen to each site for a full inspiration and expiration cycle.
• Have patients breathe in and out slowly through their mouth. Let the patient set the pace and prevent hyperventilating patients with respiratory disorders like COPD.
• When assessing breath sounds EMTs should listen for pitch, quality, volume, duration of respirations, and any adventitious lung sounds.
• Use the diaphragm of the stethoscope directly on the patient’s skin. Clothing can make noises like adventitious lung sounds and diminish breath sound quality.
• Don’t be afraid to ask female patients to lift or raise breast tissue if you need to auscultate lung sounds. Listening over breast tissue can muffle breath sounds.
• Use the auscultation sites pictured above as a guide to finding the correct lung auscultation sites. Depending on the patient, you may need to move your stethoscope around the area to avoid tissue or bone and hear airflow movement.
• Having the patient pull their arms forward can separate the shoulder blades and help with the posterior assessment.
Extra Tips
 → If you go below the sixth intercostal space during anterior auscultation, you will begin to hear intestinal sounds instead of breath sounds.
→ If you go below the sixth intercostal space during anterior auscultation, you will begin to hear intestinal sounds instead of breath sounds.
→ The posterior chest is preferred for lung auscultation because there are fewer bones and muscles to disperse sounds.
→ Listen to breath sounds on every patient you can if you want to become experienced at this skill. Becoming familiar with clear breath sounds will make you better at picking up on adventitious lung sounds when they are present.
Looking for more EMT topics? Check out:
⇒ A Guide to Pediatric Vital Signs by Age
⇒ Ten Best EMS Boots & A Guide to Choosing Work Boots
⇒ Prehospital Care of Electrocution Injuries
⇒ 35 Great Books for EMTs and Paramedics
Christina Beutler is the creator of EMT Training Base. She is a former EMT and a current Registered Nurse. Christina’s path changed after taking a Basic First Aid class while in Community College, and a career in healthcare opened up. Working as an Emergency Medical Technician led to a passion for nursing and a job working in the Intensive Care Unit and Critical Care Unit right out of Nursing School. To learn more about Christina’s story, head over to the About page.

